
Patient History: 87-year-old male with a chief complaint of AMS and weakness. Family on scene state that the patient has a history of diabetes, renal failure, CABG x3 (12 years ago), and high cholesterol.
Medications: Lantus, Simvastatin, and warfarin.
Allergies: Penicillin and Sulfa-containing medications
Vital Signs: BP 91/53, HR as shown in the 12-lead, CBG 187 mg/dL, SpO2 91% on room air, Temp 97.9 deg F (oral).
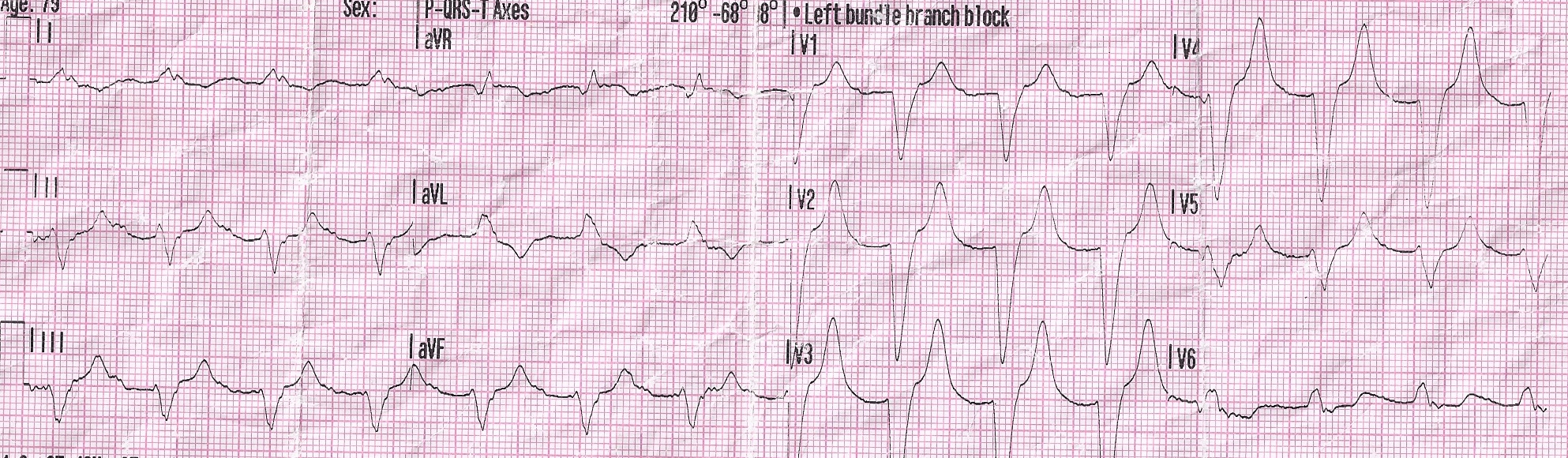
12-Lead Findings: Remember to walk through the steps we’ve outlined for you.
- Rate: Approx. 100 bpm
- Rhythm: Appears to be a regular wide complex rhythm
- Axis: -68 degrees, left axis deviations. This finding should begin to tip you off that something is not right.
- R-wave Progression: Poor. We do not see a healthy progression of negative complexes in leads V1-V2, to biphasic complexes in V3-V4, to positive complexes in V5-V6. This finding should back up your first findings in step 3 that something isn’t quite right.
- ST segment: Elevated in V1-V4.
- T-wave: Tall peaked in V2-V5, flipped in aVL. Remember, the general rule of thumb here is, “if you wouldn’t want to sit on the T-wave, something is not right.” This finding should lead you to believe we’re seeing the patient’s renal failure in action.
- Q-wave: Not present.
- Reciprocal changes: None seen.
Sick or not sick? SICK right!? If a patient’s medical condition is beginning to show up on his/her 12-lead ECG, that is most likely a late sign that something has been festering for a while. This patient was treated per local hyperkalemia protocol. The crew backed up their decision with the 12-lead ECG changes (lack of sinus P-wave, wide QRS, tall peaked T-waves) with their physical findings (altered mental status, general weakness, and history of renal failure).
- Dozens of courses and topics
- State-specific requirements
- We report to CAPCE in real time